ADENOMA DIAMETER ≥2.4 CM AND DST CORTISOL >1.8 ΜG/DL CONFER ELEVATED RISK OF HYPERCORTISOLISM.
Article Summary
Valentina Morelli, Giuseppe Reimondo, Roberta Giordano, et al. Long-term follow-up in adrenal incidentalomas: an Italian multicenter study. J Clin Endocrinol Metab. 2014;99(3):827-834. doi:10.1210/jc.2013-3527
The long-term consequences of less severe hypercortisolism in patients with adrenal adenomas are unknown.* During routine clinical testing, many patients exhibit biochemical evidence of excess cortisol secretion, but without the associated features of classically described overt Cushing syndrome.† This is referred to as hypercortisolism without Cushingoid features or less severe hypercortisolism. Less severe hypercortisolism has been linked to several health complications, including obesity, arterial hypertension, dyslipidemia, osteoporosis, and type 2 diabetes mellitus. Despite these known associations, appropriate long-term management remains unclear.
To analyze the long-term health risks associated with excess cortisol secretion, a retrospective multicenter study evaluated 206 patients with adrenal adenomas and no signs of classically described overt Cushing syndrome. Over the course of ≥5 years, patients were observed for adrenocortical function, metabolic changes, incident cardiovascular events, and adenoma size. Study results concluded that patients with adenomas ≥2.4 cm had an increased risk of developing hypercortisolism over time. Additionally, the incidence of cardiovascular events was more common in patients with less severe hypercortisolism than in those without. The findings suggested that long-term follow-up is needed for patients with adrenal adenomas ≥2.4 cm in order to monitor the risk of cardiovascular events and the development of hypercortisolism. The study also highlighted the importance of considering the increased risk of cardiovascular events when choosing treatment options for patients with less severe hypercortisolism.
In this study, patients were considered to have less severe hypercortisolism if post-dexamethasone suppression test (DST) cortisol levels were >5 μg/dL, or if they had at least 2 of the following: urinary-free cortisol greater than the upper limit of normal; low adrenocorticotropic hormone (ACTH <10 /pg/mL); or post-DST cortisol levels >3 μg/dL.
†Biochemical evidence = lab results.
Annual rate of CV events higher in patients with hypercortisolism
- Retrospective, multicenter study analyzing 206 patients with adrenal adenomas. Follow-up time of ≥5 years (median: 72.3 months; range: 60 to 186 months)
- In this study, patients were considered to have hypercortisolism if post-DST cortisol levels were >5 μg/dL, or if they had at least 2 of the following: urinary-free cortisol greater than the upper limit of normal; low ACTH (<10 pg /mL); or post-DST cortisol levels >3 μg/dL
Rate of cardiovascular events
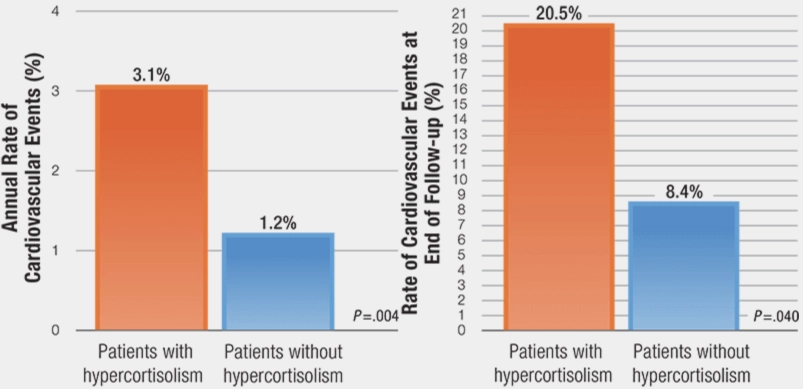
Bar chart showing that the annual rate of cardiovascular events was 3.1% in patients with hypercortisolism, compared with 1.2% in patients without hypercortisolism.
Bar chart showing that the rate of cardiovascular events at end of follow-up was 20.5% in patients with hypercortisolism, compared with 8.4% in patients without hypercortisolism.
- Patients with hypercortisolism were 2.7 times more likely to experience new CV events during the follow-up period
- Patients with hypercortisolism at baseline were 3.1 times more likely to have had a previous CV event than those without hypercortisolism at baseline
- The same analysis showed that patients with type 2 diabetes at baseline were 2 times more likely to have had a previous CV event than those without type 2 diabetes at baseline
- At the end of follow-up, patients with hypercortisolism had a higher prevalence of arterial hypertension and type 2 diabetes than patients without hypercortisolism
Adrenal adenoma size ≥2.4 cm associated with increased risk of developing hypercortisolism
- Over the study period, 8.2% of patients with adrenal adenomas developed hypercortisolism, the risk being particularly increased in patients with an adenoma size ≥2.4 cm
- Those with adenomas ≥2.4 had an increased risk of CVD
Development of hypercortisolism based on adrenal adenoma size

Four of the 105 patients (3.8%) without hypercortisolism at baseline and with an adenoma <2.4 cm developed hypercortisolism during follow-up.
†Eleven of the 77 patients (14.3%) without hypercortisolism at baseline and with an adenoma ≥2.4 cm developed hypercortisolism during follow-up.
- Patients were excluded from the study if they had psychiatric diseases; history of alcoholism or drug use; signs of classically described overt Cushing syndrome; or a history of malignancy, infections, adrenal hemorrhage, pheochromocytoma, primary hyperaldosteronism, or an infiltrative disease that could potentially affect the adrenal glands
- The mean follow-up time for patients was 82.5±32 months, ranging between 60 and 186 months
- Patients with hypercortisolism were 2.7 times more likely to experience new cardiovascular events during the follow-up period
- The annual rate of cardiovascular events was higher in patients with less severe hypercortisolism than in those without less severe hypercortisolism, at 3.1% and 1.2%, respectively
- Patients with type 2 diabetes at baseline were 2 times more likely to have had a previous cardiovascular event than patients without type 2 diabetes at baseline, whereas patients with less severe hypercortisolism at baseline were 3.1 times as likely to have had a previous cardiovascular event than patients without less severe hypercortisolism at baseline
- At the end of follow-up, patients with less severe hypercortisolism had a higher prevalence of arterial hypertension and type 2 diabetes than patients without less severe hypercortisolism