Article Summary
Cardiovascular events and mortality in patients with adrenal adenomas and excess cortisol secretion
Guido Di Dalmazi, Valentina Vicennati, Silvia Garelli, et al. Cardiovascular events and mortality in patients with adrenal incidentalomas that are either non-secreting or associated with intermediate phenotype or subclinical Cushing’s syndrome: a 15-year retrospective study. Lancet Diabetes Endocrinol. 2014;2(5):396-405. doi:10.1016/S2213-8587(13)70211-0
The discovery of adrenal adenomas associated with hypercortisolism has increased over the last few years. It’s a common finding for patients with these adrenal adenomas to have autonomous cortisol secretion with lack of Cushingoid features, also referred to as less severe hypercortisolism when compared with classically described overt Cushing syndrome.* Although metabolic alterations and increased cardiovascular risk have been noted in patients who have autonomous cortisol secretion with lack of Cushingoid features, incidence of cardiovascular events and mortality in the long term have not been assessed.
To date, no studies have been done to assess cardiovascular risk and mortality in patients with adrenal adenomas and less severe hypercortisolism. To bridge this gap, a retrospective study was conducted using data from 1995 to 2010 to analyze the correlation between excess autonomous cortisol secretion, cardiovascular issues, and mortality. The 15-year study looked at the frequency of new cardiovascular events and mortality in patients with adrenal adenomas and hypercortisolism. These were categorized based on post-dexamethasone suppression test (DST) cortisol levels. The analysis, which excluded patients with classically described overt Cushing syndrome, found that cardiovascular events, as well as mortality rates, were higher in patients with increased cortisol levels over a period of time. Additionally, post-DST amounts of cortisol are related to all-cause mortality independently of all potential risk factors considered.
Units of measurement have been converted from the International System of Units (µg/dL) to traditional units (ug/dL) using the standard endocrinology conversion factor for cortisol levels.
Hypercortisolism is associated with significant clinical consequences, including morbidity and mortality
- 15-year, retrospective, single-center study analyzing 198 consecutive patients with adrenal adenomas. Individuals were assessed every 18 to 30 months for the first 5 years. Mean follow-up period was 7.5 years (range: 26 months to 15 years)
- Patients were grouped based on their post-DST cortisol levels at baseline and at study end
Patients who were diagnosed with classically described overt Cushing syndrome were excluded from the study.
Worsening cortisol secretion patterns over time
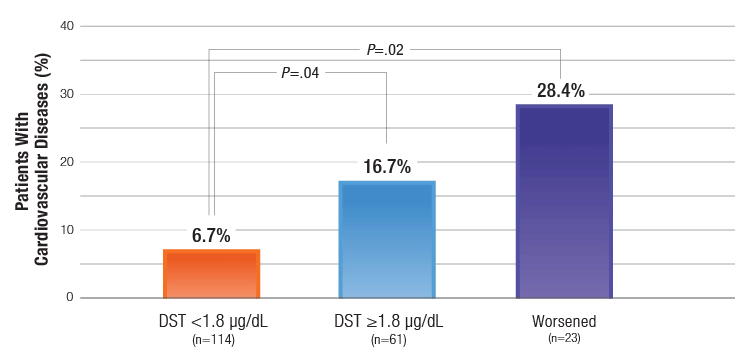
- At the end of follow-up, patients with DST ≥1.8 μg/dL, and those with a worsened secretion pattern had a higher incidence of CVD than patients with DST <1.8 μg /dL
- Post-DST cortisol levels related to all-cause mortality independently of all other risk factors
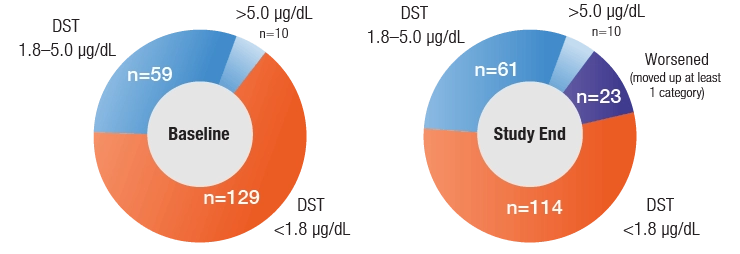
DST=dexamethasone suppression test.
Incidence of new cardiovascular events* at the end of follow-up
DST=overnight dexamethasone suppression test.
New cardiovascular events were defined as nonfatal acute myocardial infarction, percutaneous transluminal coronary angioplasty, and surgical bypass for ischemic heart disease, or ischemic stroke, which occurred during the study.
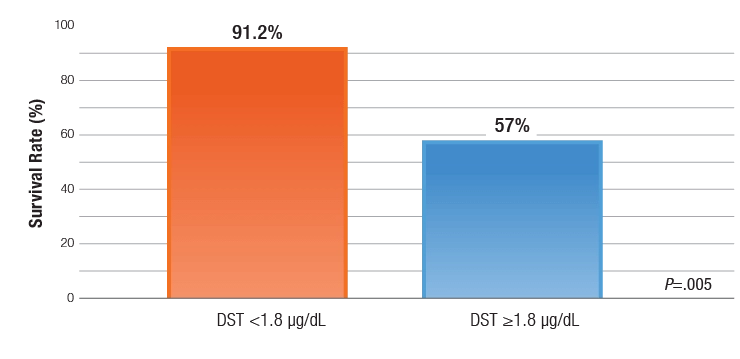
Survival rates for all-cause mortality in patients with adrenal adenomas at the end of follow-up
DST=dexamethasone suppression test.
- Patients who were diagnosed with classically described overt Cushing syndrome were excluded from the study
- Mortality rates were higher for patients who had stable excess levels of cortisol secretion or increasing levels of cortisol secretion over time
- Post-DST cortisol levels related to all-cause mortality independently of all other risk factors
- The survival rate for all-cause mortality in patients with DST ≥1.8 μg/dL was 57% compared with 91.2% in those with DST <1.8 μg /dL