Article Summary
Effects of cortisol levels on mortality rates in patients with adrenal adenomas
Miguel Debono, Mike Bradburn, Matthew Bull, Barney Harrison, Richard J. Ross, John Newell-Price. Cortisol as a marker for increased mortality in patients with incidental adrenocortical adenomas. J Clin Endocrinol Metab. 2014;99(12):4462-4470. doi:10.120/jc.2014-3007
Adrenocortical adenomas, also known as adrenal adenomas, are found on approximately 4.5% of all computed tomography scans. On routine clinical testing, many patients exhibit biochemical evidence of excess cortisol secretion, but without the associated features of classically described overt Cushing syndrome.* This is referred to as hypercortisolism without Cushingoid features, or less severe hypercortisolism.† Previous studies have linked classically described overt Cushing syndrome to an increase in cardiovascular events and mortality. Other studies have determined that even less severe forms of hypercortisolism can lead to insulin resistance, hypertension, and visceral obesity. Therefore, it is essential to understand the significance of cortisol management in these patients. This study hypothesized that patients with adrenal adenomas and hypercortisolism may have an increased risk of cardiovascular events and mortality, even without exhibiting the phenotypic features associated with classically described overt Cushing syndrome. Moreover, the study explored how higher or lower levels of cortisol secretion affect mortality rates in these patients.
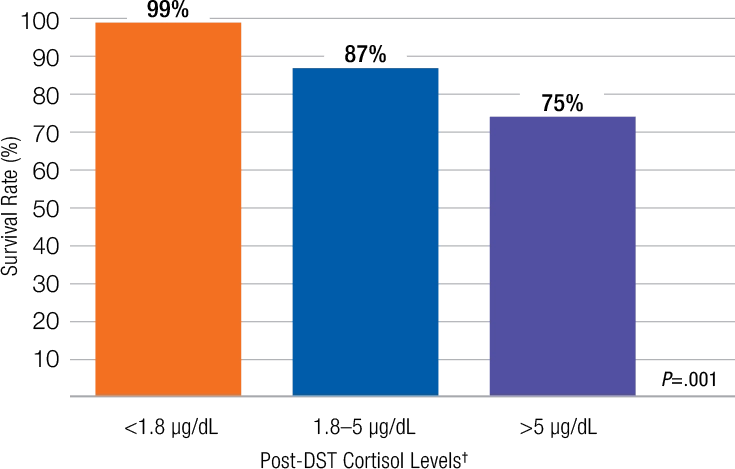
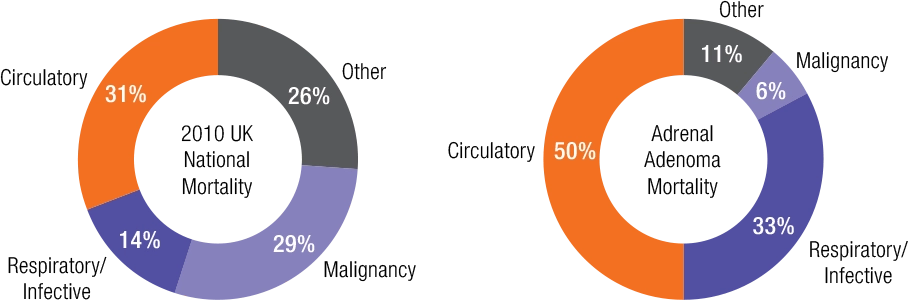
To explore this, the mortality rates of patients with adrenal adenomas and various levels of cortisol secretion were studied over an 8-year retrospective analysis. At the baseline of the study, patient cortisol levels were assessed using the overnight dexamethasone suppression test (DST), which detects autonomous cortisol secretion in the blood. The study then compared this data with the published mortality rates locally in Sheffield and nationally across the United Kingdom. Study results demonstrated a link between cortisol levels and mortality rate, concluding that patients with hypercortisolism (post-DST >1.8 μg/dL) have greater mortality. Additionally, study findings revealed a higher rate of mortality from circulatory and respiratory infection causes for patients with adrenal adenomas and evidence of hypercortisolism based on the DST.
Biochemical evidence = lab results.
†In this study, patients were considered to have less severe hypercortisolism if post-dexamethasone suppression test (DST) cortisol levels were >5 μg/dL, or if they had at least 2 of the following: urinary-free cortisol greater than the upper limit of normal; low adrenocorticotropic hormone (ACTH <10 /pg/mL); or post-DST cortisol levels>3 μg/dL.
DST=dexamethasone suppression test.
‡Chart data taken from Figure 2A in article. Median observation time was 4.2 years.
§Post-DST cortisol levels categorized using standard cutoffs from literature.
- The retrospective study analyzed 206 patients who were diagnosed with adrenal adenomas between January 2005 and July 2013
- Screening for hypercortisolism was conducted using the 1-mg overnight DST
- Post-DST cortisol cutoff of >1.8 μg/dL is in keeping with a diagnosis of cortisol excess as recommended by Endocrine Society guidelines
- Patients were classified into 3 groups based on cortisol levels after undergoing a DST, according to cortisol excess guidelines recommended by the Endocrine Society, which included:
- Post-DST cortisol
<1.8 μg /dL
- Post-DST cortisol
1.8–5 μg/dL
- Post-DST cortisol
>5 μg/dL
- Patients with adrenal adenomas who fail to suppress serum cortisol on DST have greater mortality, which increases as post-DST cortisol level increases
Causes of Mortality in Patients With Adrenal Adenomas Compared With National Average
Patients were excluded from the study if they had a suspected malignancy, classically described overt Cushing syndrome, worsening metabolic features, an adenoma >4 cm in diameter or demonstrated increase in size at 6-month follow-up, or the phenotype for Cushing syndrome
Patients were referred to the Endocrine Investigation Unit of Royal Hallamshire Hospital, Sheffield Teaching Hospitals National Health Service Foundation Trust in Sheffield, UK within 6 months of a physician detecting the initial adenoma
Causes of mortality were grouped according to the following:
- Circulatory diseases(including ischemic heart disease, hypertensive heart disease, cerebrovascular disease, congestive heart failure, and atherosclerotic vascular disease)
- Respiratory disease and infection
- Malignancy
- Other